flowchart LR
subgraph IP["Infection Process"]
A[Residential segregation] --> B(Isolation)
A --> C(Concentration)
C --> D{Infection <br> Inequity}
B --> D
end
subgraph MP["Mortality Process"]
D --> E((Case Fatality <br> Rate))
E --> F{Mortality <br> Inequity}
B --> G(Healthcare <br> Access/Quality)
G .->
I(Comorbidity <br> Prevalence) .-> E
end
H{{Structural Racism}} --> A
H --> G
H --> I
style IP fill:none
style MP fill:none
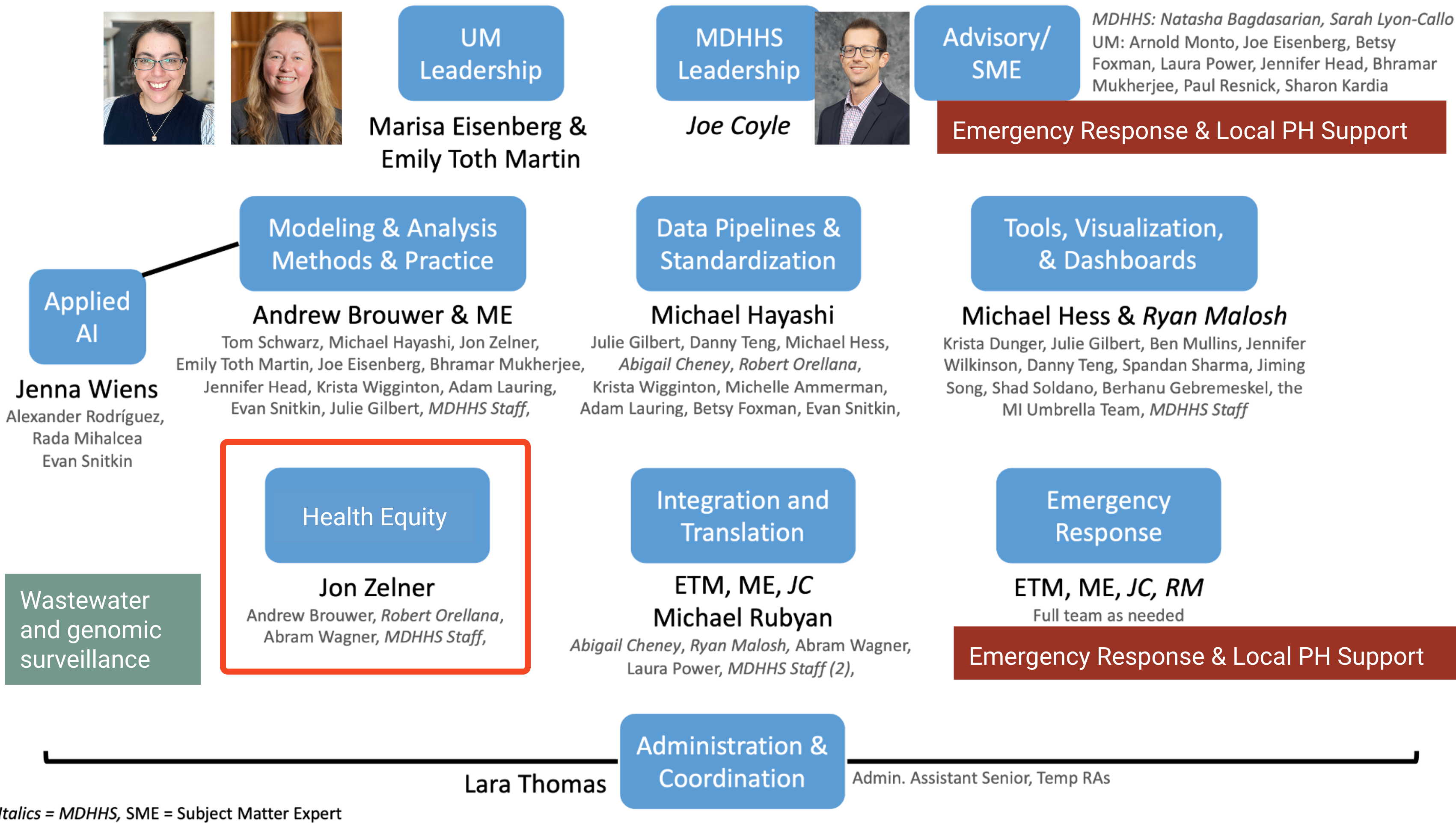
Modeling to support health equity in Michigan
A systems of exposure approach
MICOM Site Visit
University of Michigan
2024-05-22
Jon Zelner
Dept. of Epidemiology
Center for Social Epidemiology and Population Health
University of Michigan School of Public Health
✉️ jzelner@umich.edu
🌐 epibayes.io

![]()
Health Equity: A pillar? 🏗️ A cloud? ☁️ A web? 🕸️
In the wake of the COVID-19 pandemic there has been a proliferation of conceptual frameworks linking socio-structural inequity to infection outcomes.
These are implicitly or explicitly rooted in the fundamental cause approach
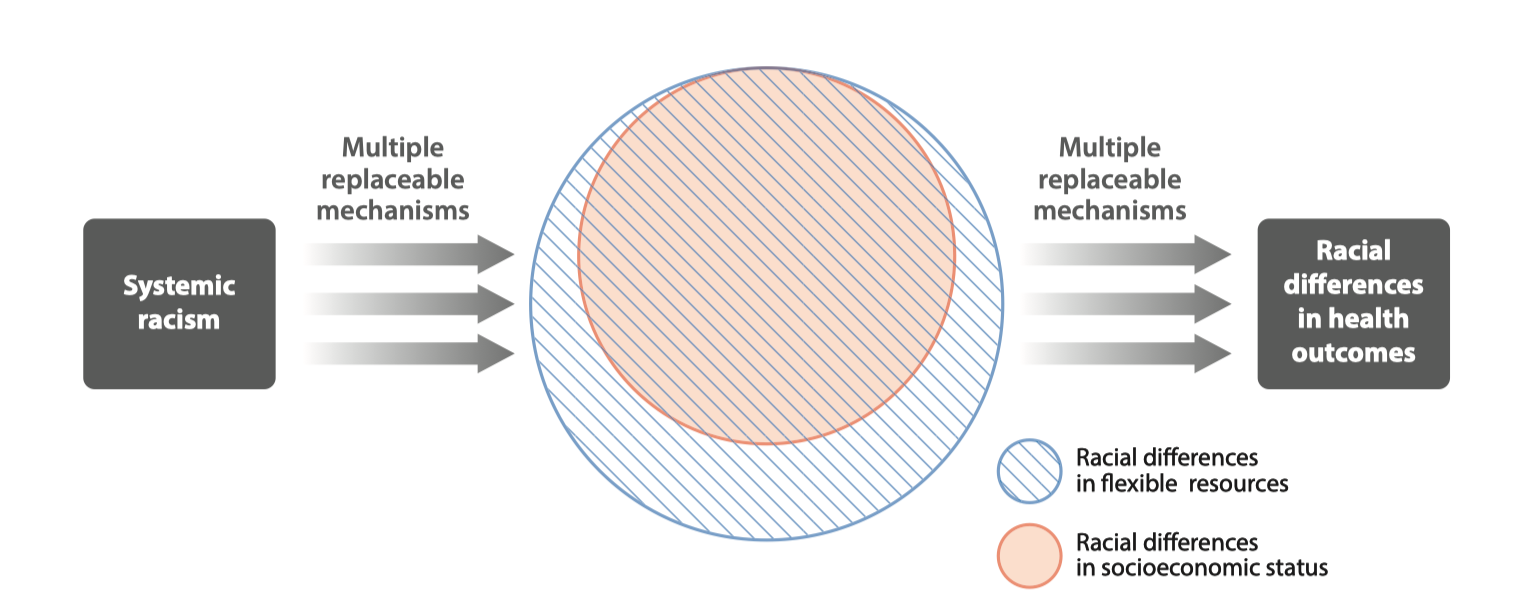
Conceptual model of racism as a fundamental cause of health inequity (From Phelan and Link (4))
Wait, I thought innovation was a good thing?
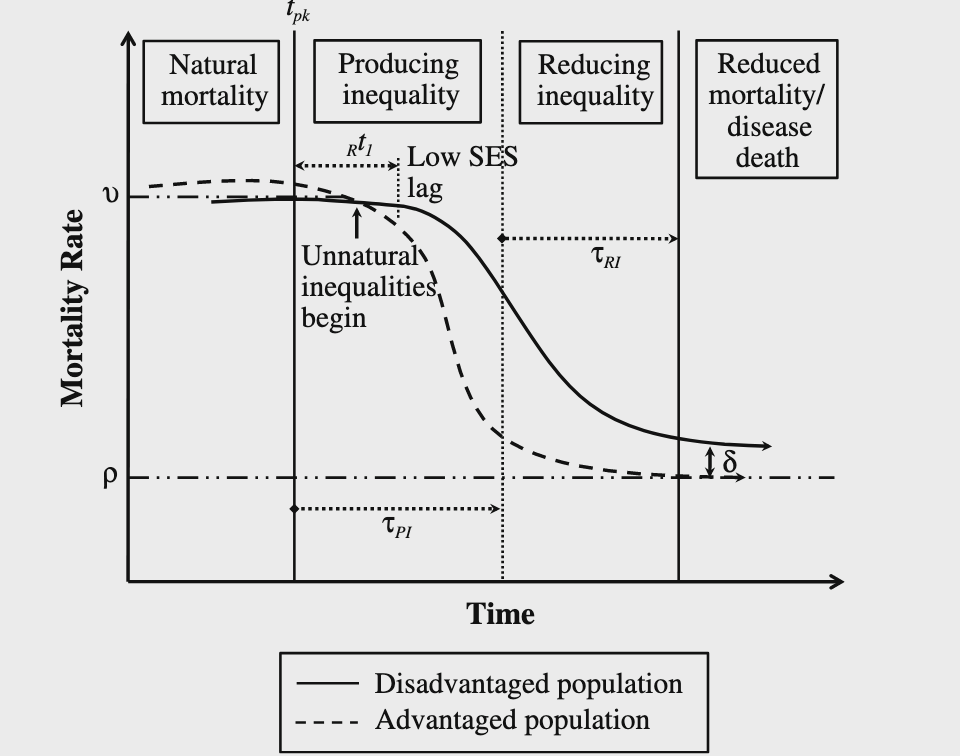
Innovations that diffuse along SES gradients may inadvertently increase inequity by providing early access to those who are most advantages (Figure from Clouston (2016) (5))
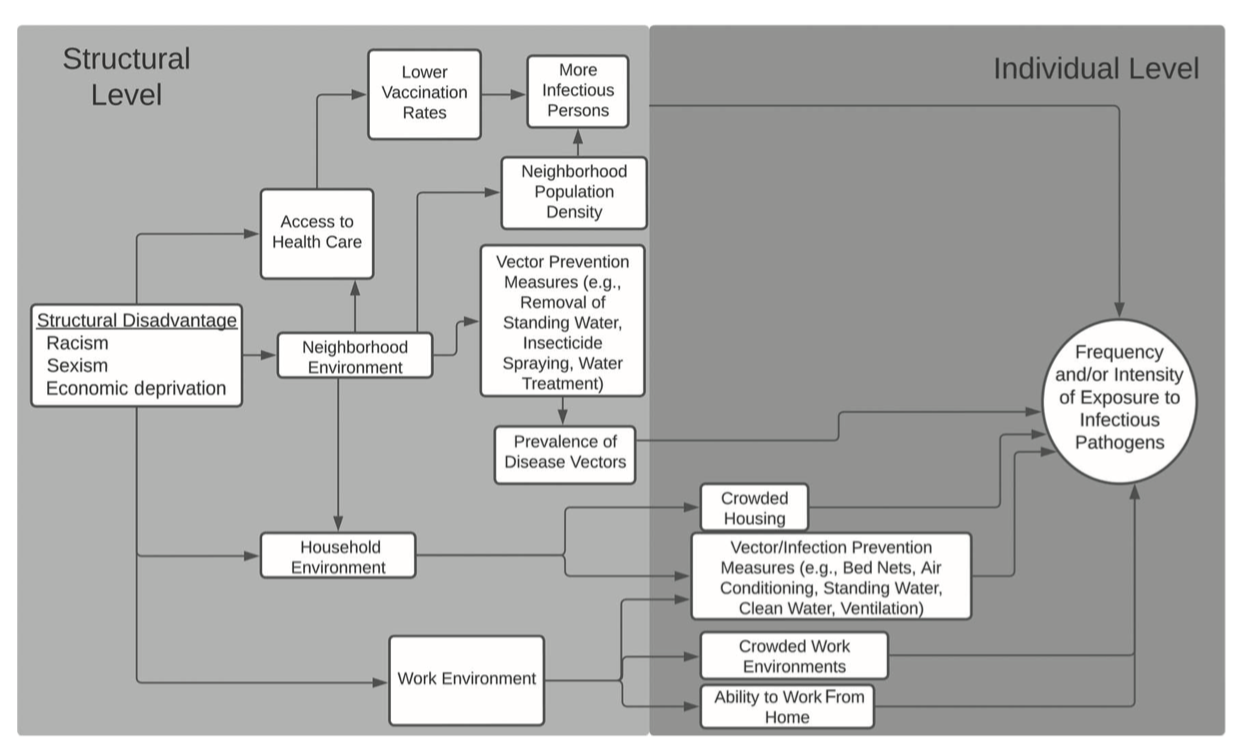
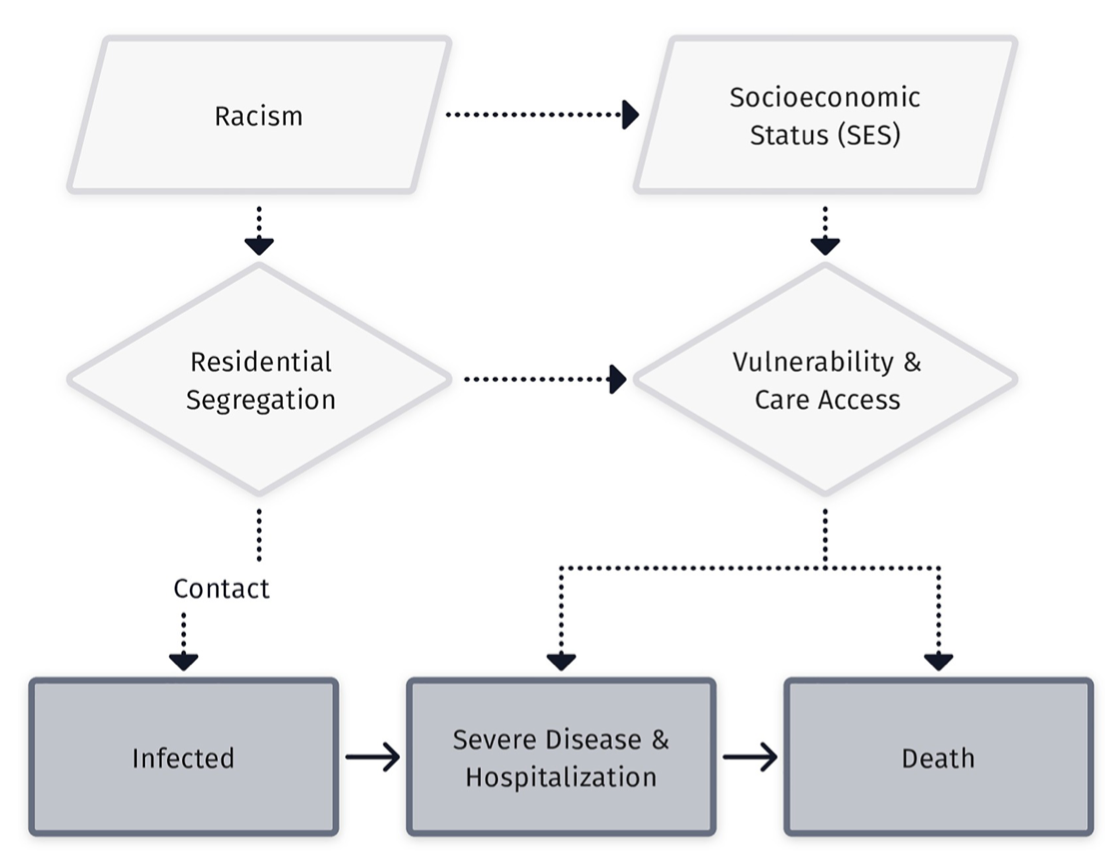
Fundamental causes orcheastrate infection inequity via systems of exposure
Riley (6) describes these systems in general terms relating to environmental exposure, social stress, differential treatment and so on.
In the context of infectious disease, this is about who gets exposed, when, and what happens to them when they are ill.
Requires a new approach to both transmission and statistical modeling (7).
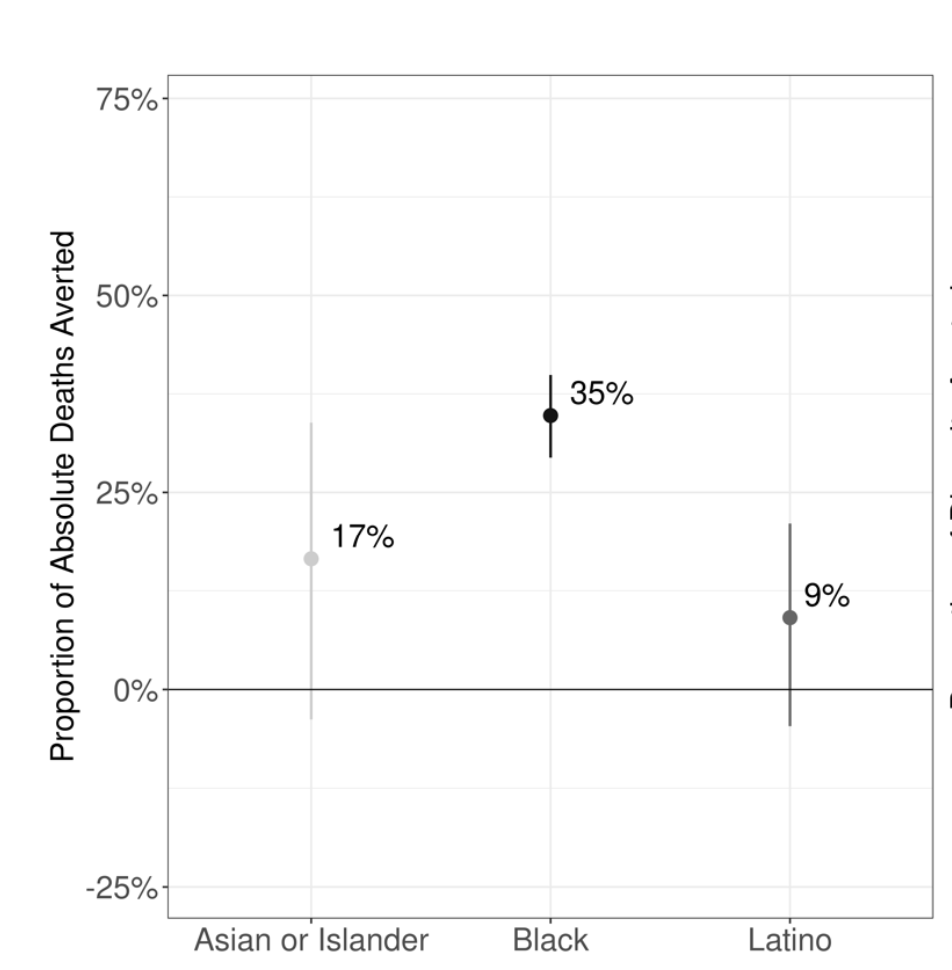
Case example: What explains time-varying patterns of SARS-CoV-2 mortality in Michigan during 2020?
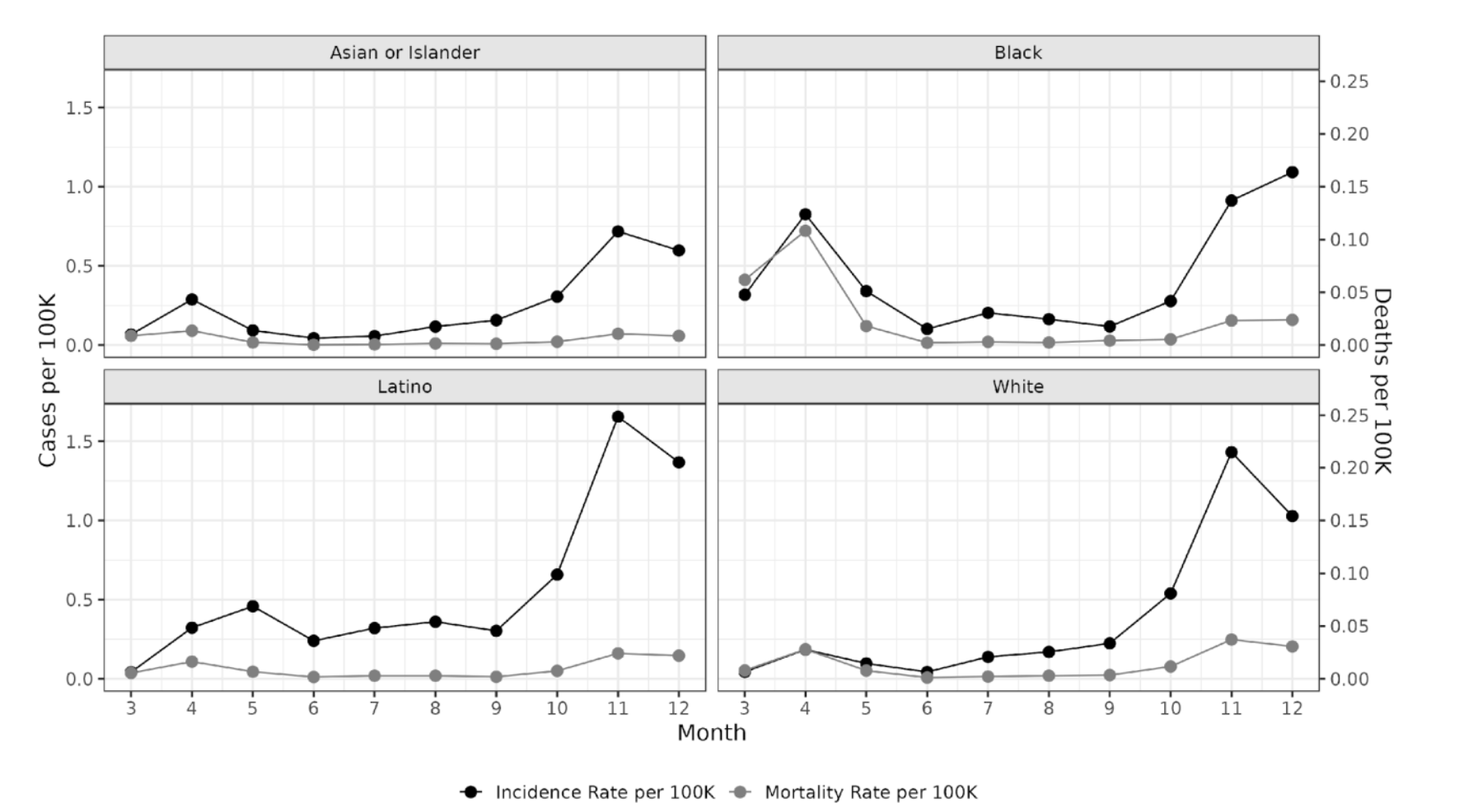
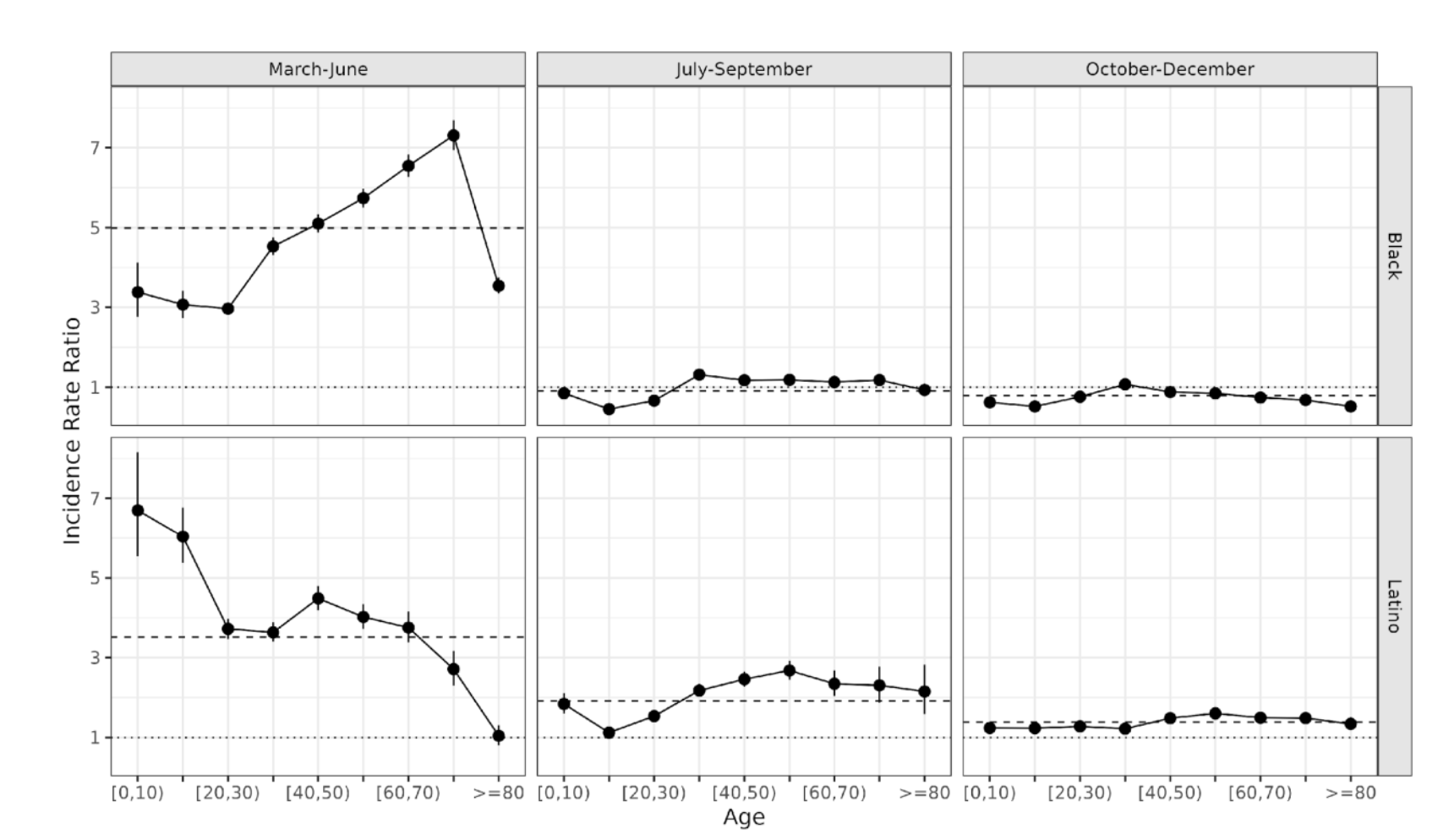
Differential incidence and mortality rates by race/ethnicity and month of 2020 (From Naraharisetti et al. Under Review.)
Case-fatality rates varied much more over time than they did between groups
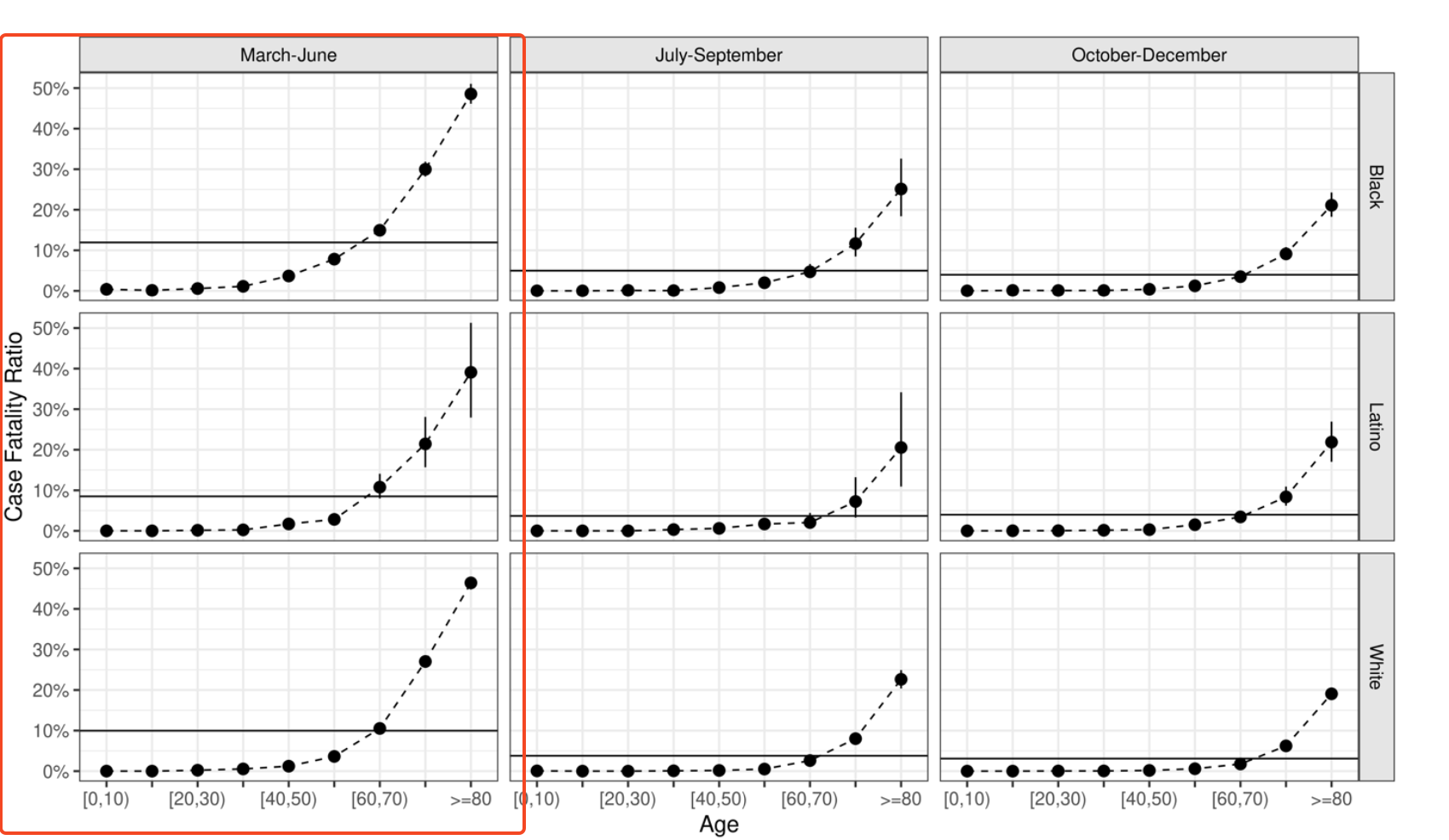
Relative risks of infection were much greater in the first period than later periods
Infection timing matters
We can’t respond our way out of this type of outcome.
Our modeling efforts have to account for the structural preconditions to inequity in emerging infection risk.
But: We also have to be prepared for best- and wort-case scenarios in order to minimize and mitigate these inequities when they arise.