flowchart LR
AA{{Structural Racism}} --> A
A[Residential segregation] --> B(Spatial Dissimilarity)
A --> C(Increased vulnerability)
C --> D{Infection <br> Inequity}
B --> D
Spatial process or social residue?
Modeling the joint socio-structural and spatial drivers of infection inequity
Statistical Methods for Infectious Disease Across Scales
Penn State University
2024-04-05
Jon Zelner
Dept. of Epidemiology
Center for Social Epidemiology and Population Health
University of Michigan School of Public Health
✉️ jzelner@umich.edu
🌐 epibayes.io
![]()
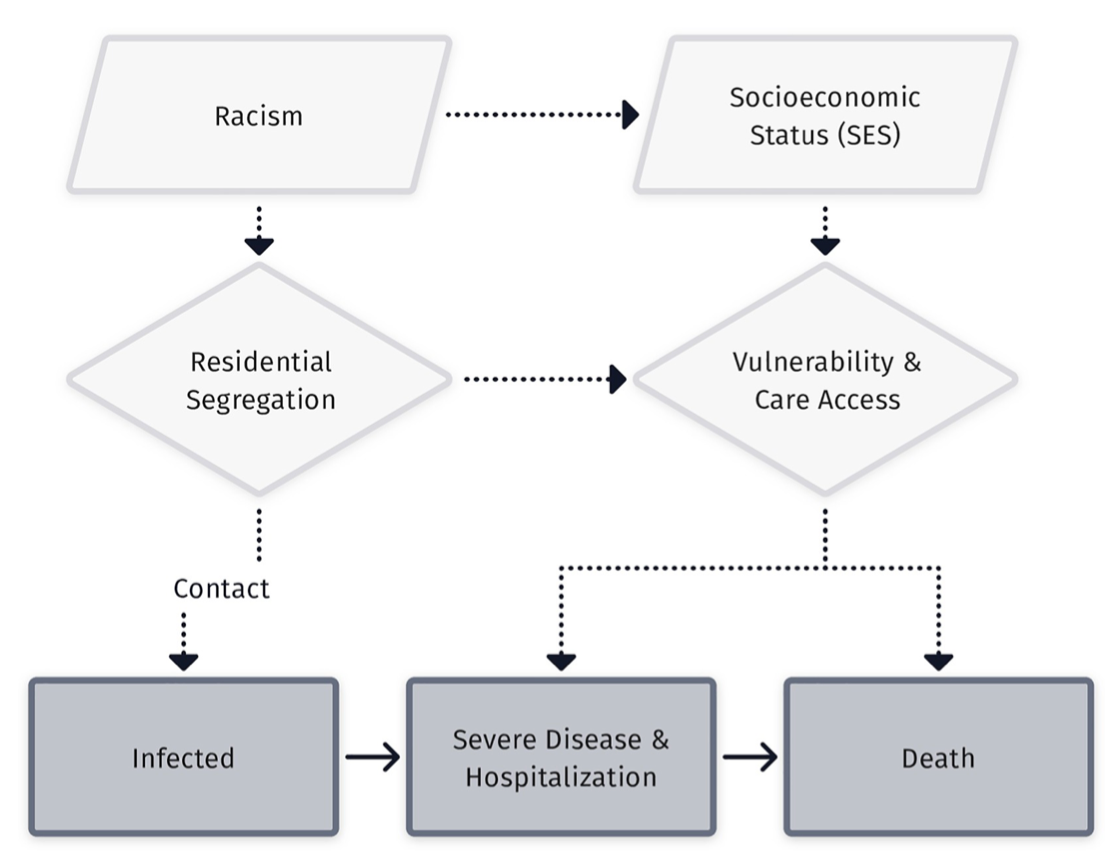
In the wake of the COVID-19 pandemic there has been a proliferation of conceptual frameworks linking socio-structural inequity to infection outcomes.
These are implicitly or explicitly rooted in the fundamental cause approach
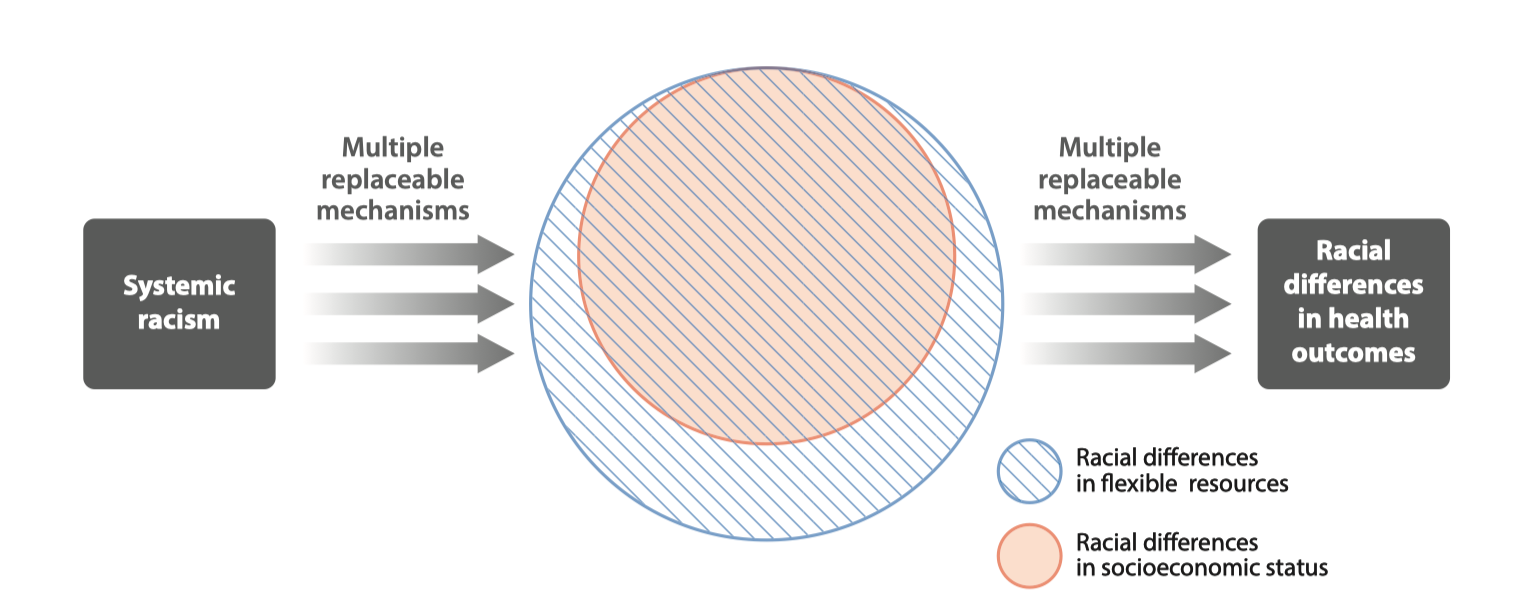
Conceptual model of racism as a fundamental cause of health inequity (From Phelan and Link (4))
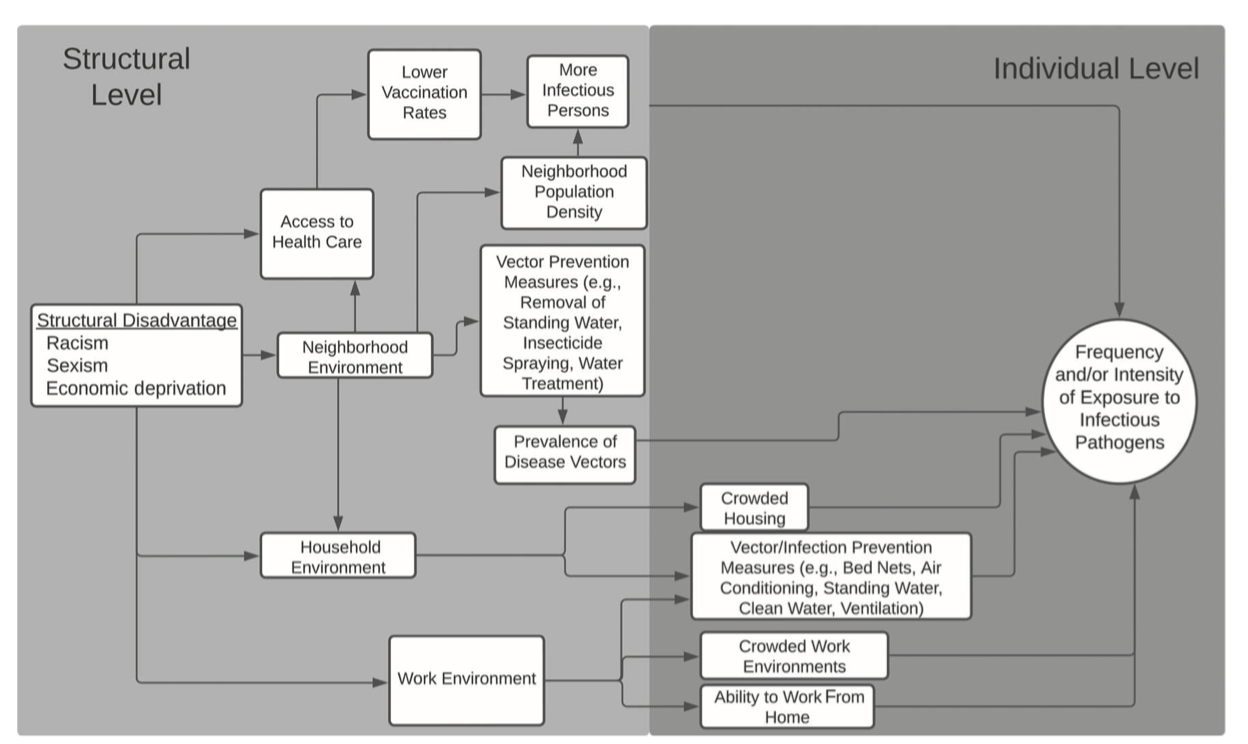
Residential segregation is a fundamental cause of health inequities that is related to but distinct from racism
Segregation restricts access to healthcare and health-promoting physical environments.
Inequity in purchasing power due to artificially inflated housing, food and other costs.
Increased risk of crime victimization, overpolicing, and police violence.
How to apply this thinking to infectious disease transmission is still very much an open question.
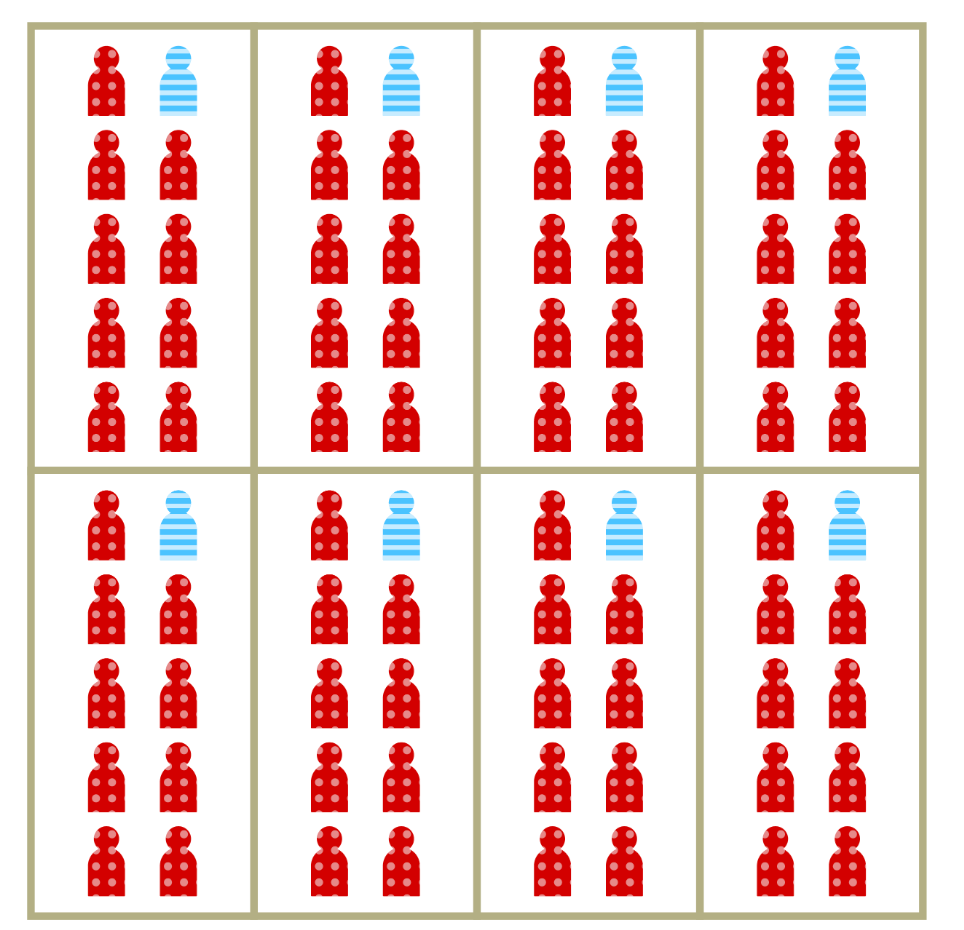
Segregation is a general process that goes beyond race and socioeconomic status

Example of spatial separation of Hindus and Muslims in Mumbai from Susewind (6)
Segregation is a multidimensional process
Spatial separation is the most obvious feature of segregation.
Often captured by metrics of clustering or spatial distributiuon including dissimilarity and Moran’s I.
When we conflate separation with vulnerability, we risk attributing the wrong spatial causes to disparities in infection outcomes.
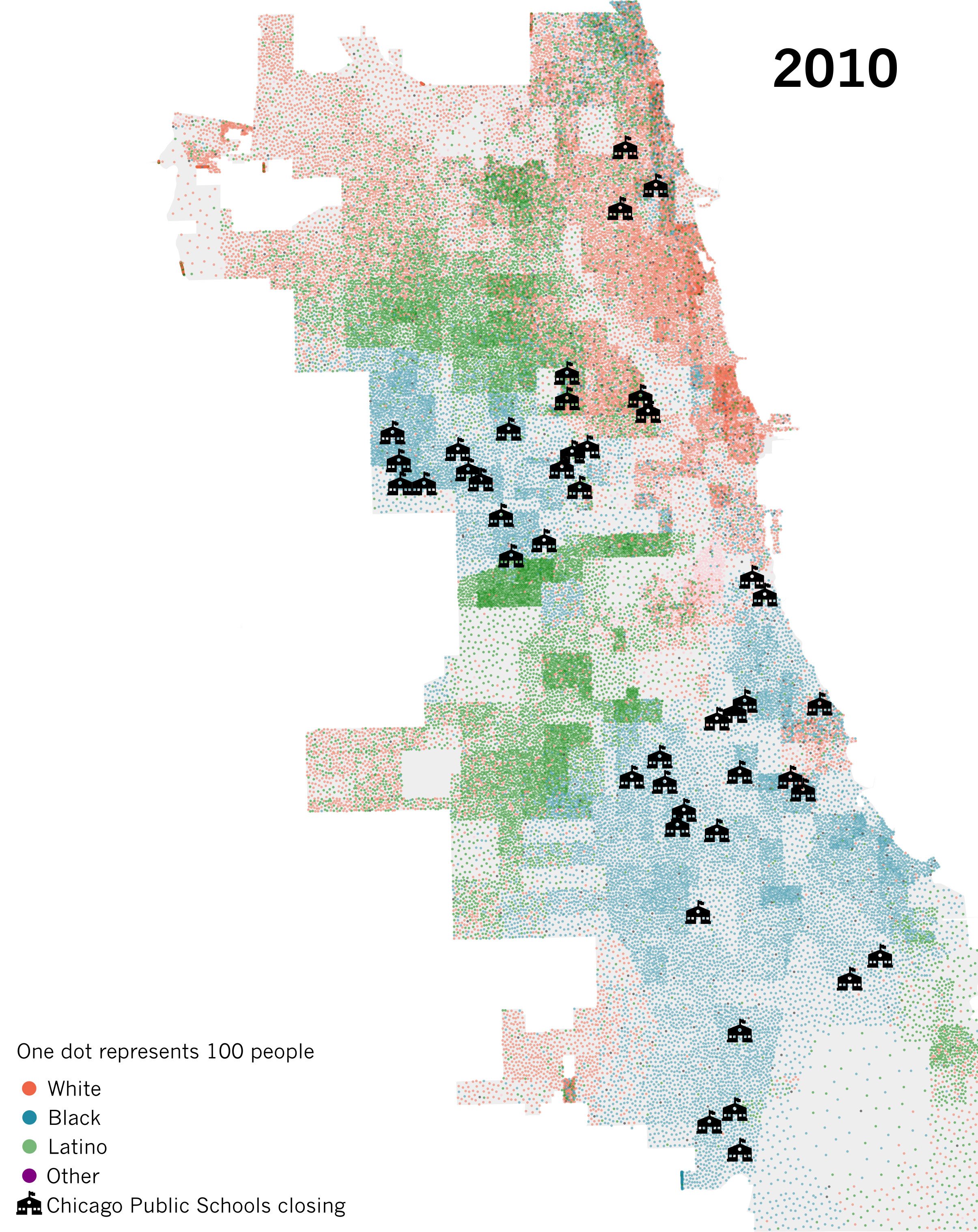
Spatial separation is a hallmark of segregation
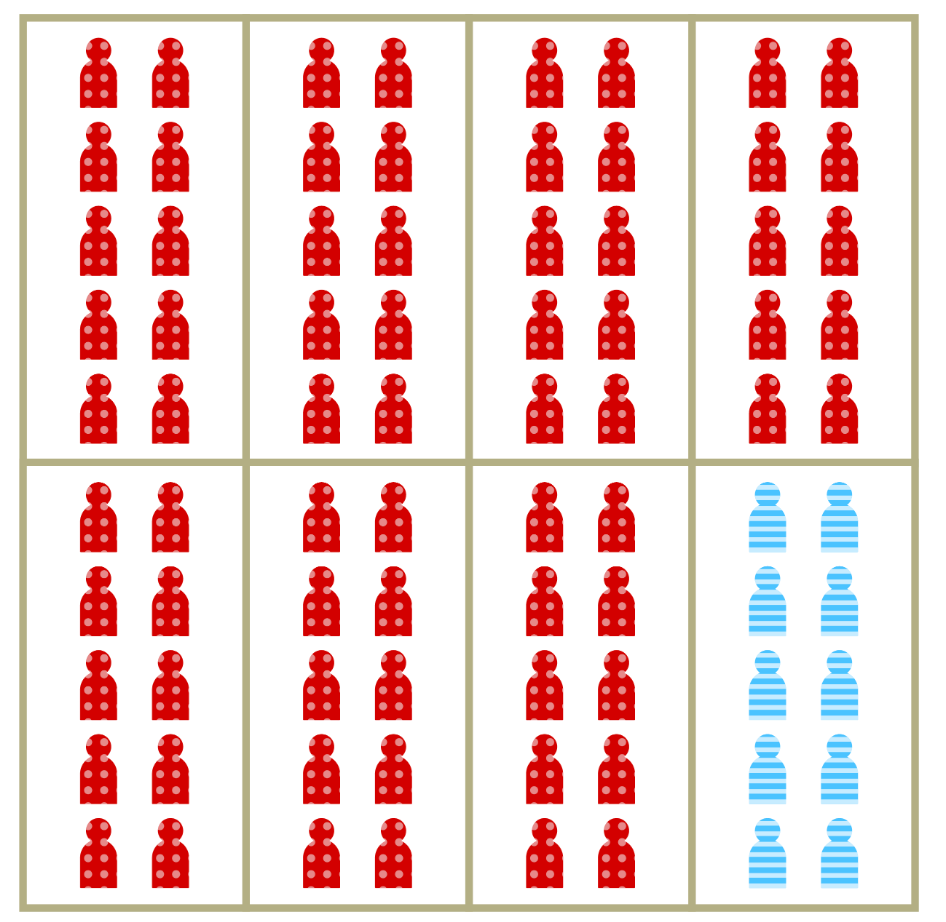
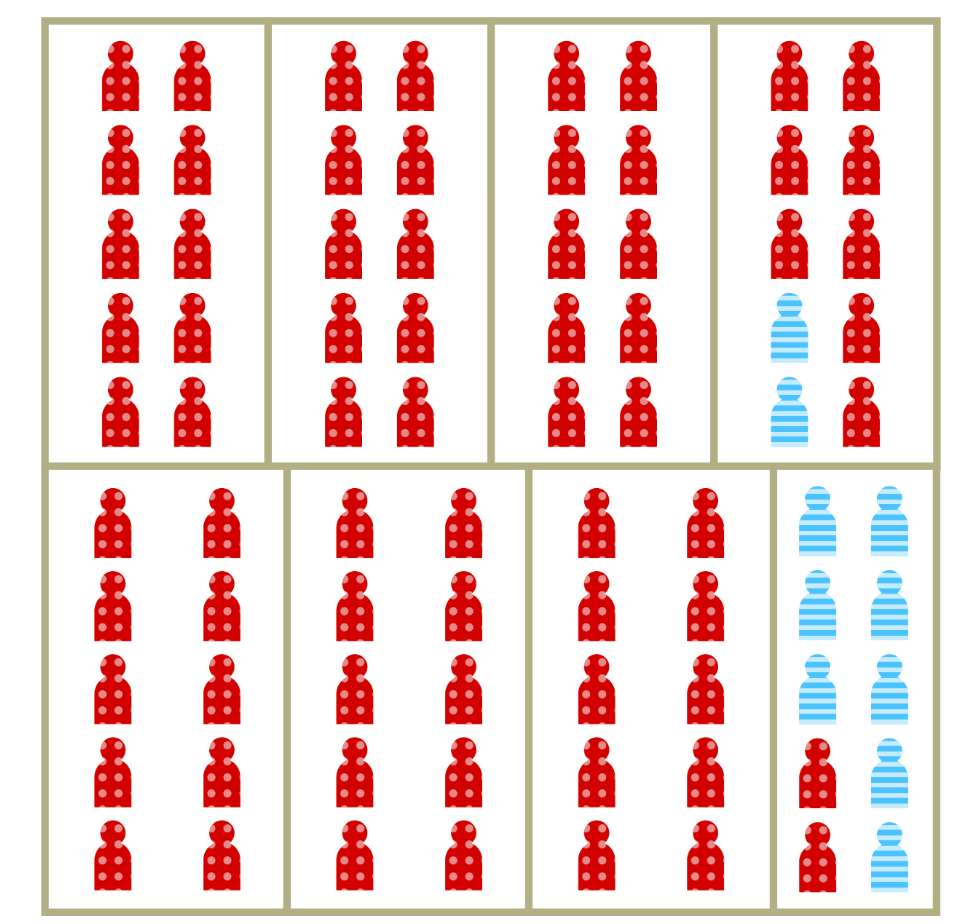
- Dissimilarity measures the proportion of members of the minority group who would have to move to achieve proportional mixing.
- Commonly used to measure spatial segregation in demographic and disease data.
- Measure is independent of density.
- Random mixing occurs in the situation dissimilarity = 0, no mixing when dissimilarity = 1
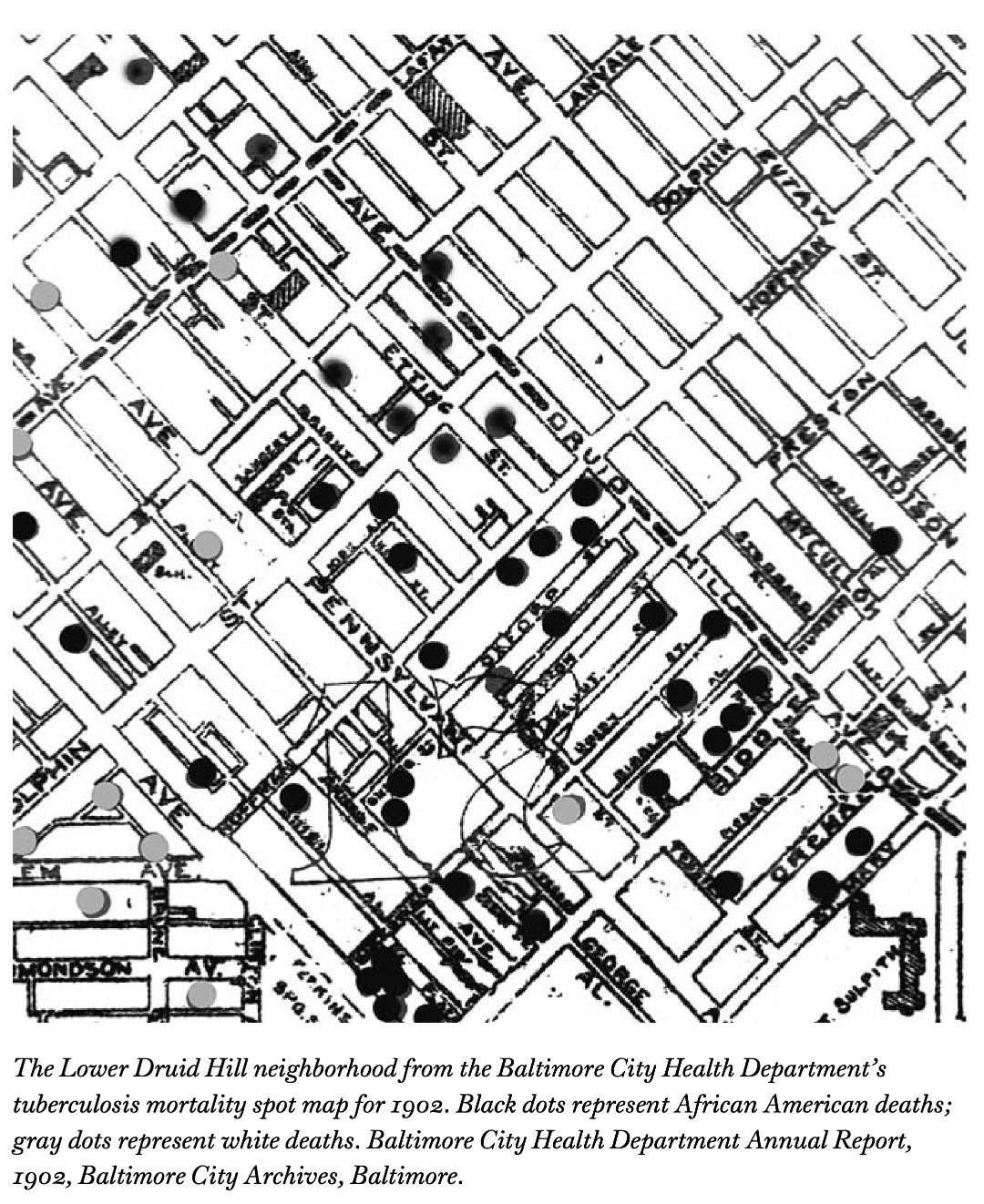
Increased vulnerability is a less visible aspect of segregation
Represents the relative increase in per-contact risk of infection among members of segregated populations.
Can also be thought of as relative vulnerability to infection.
May result from household crowding, increased occupational risk, comorbidities and other factors
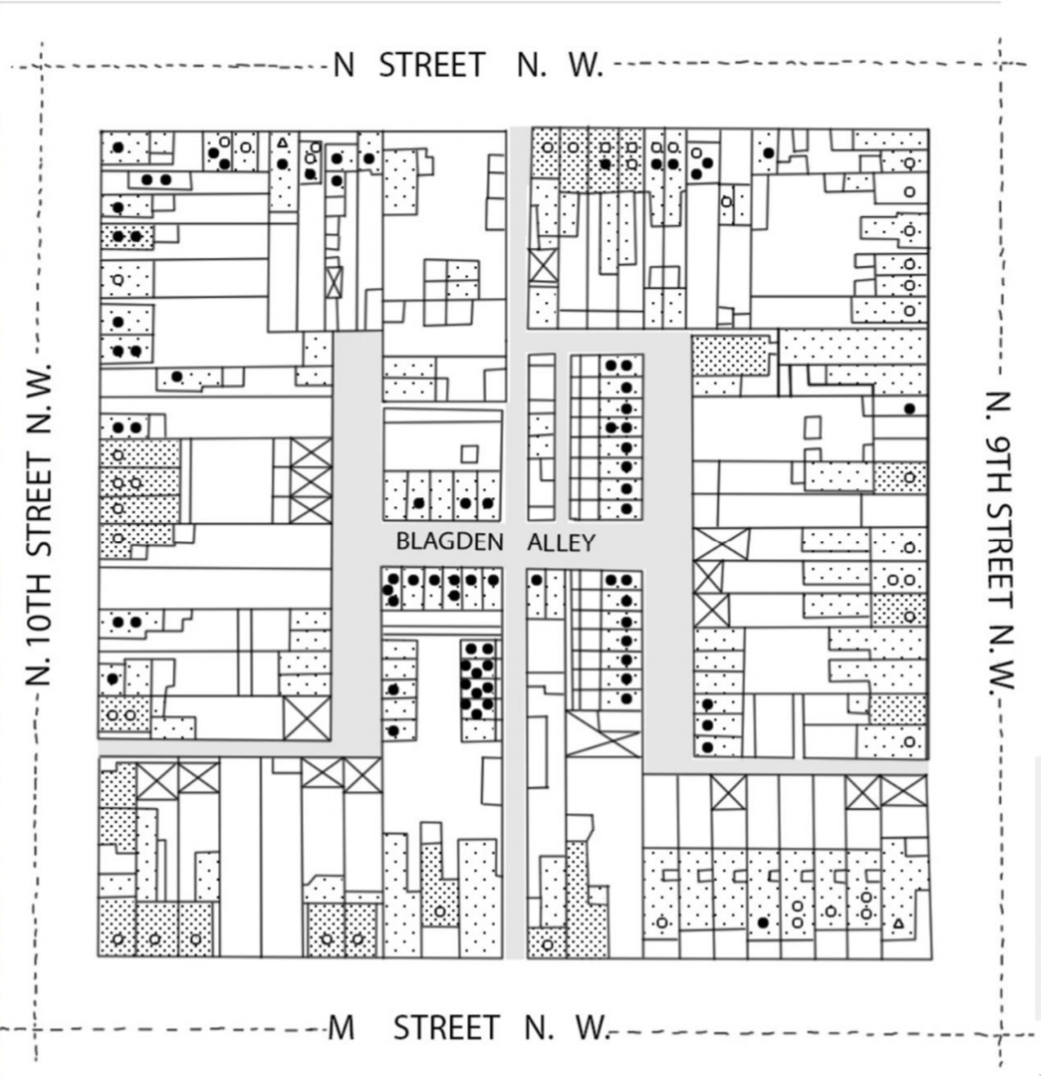
Lage-scale separation isn’t necessary for segregation to drive inequity in risk
Time for the the rubber to meet the road! 🔥

As a public employee of the state of Michigan, I am contractually obligated to include at least 1 (one) automotive metaphor per talk.
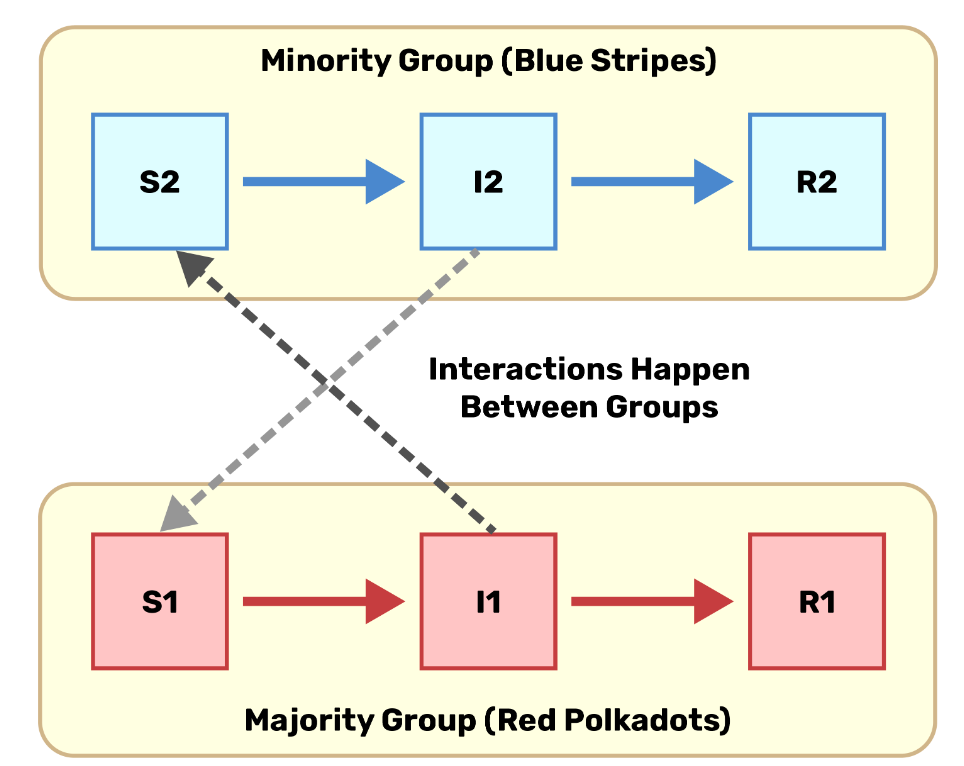
We’ll use a simple model to chip away at this complex problem
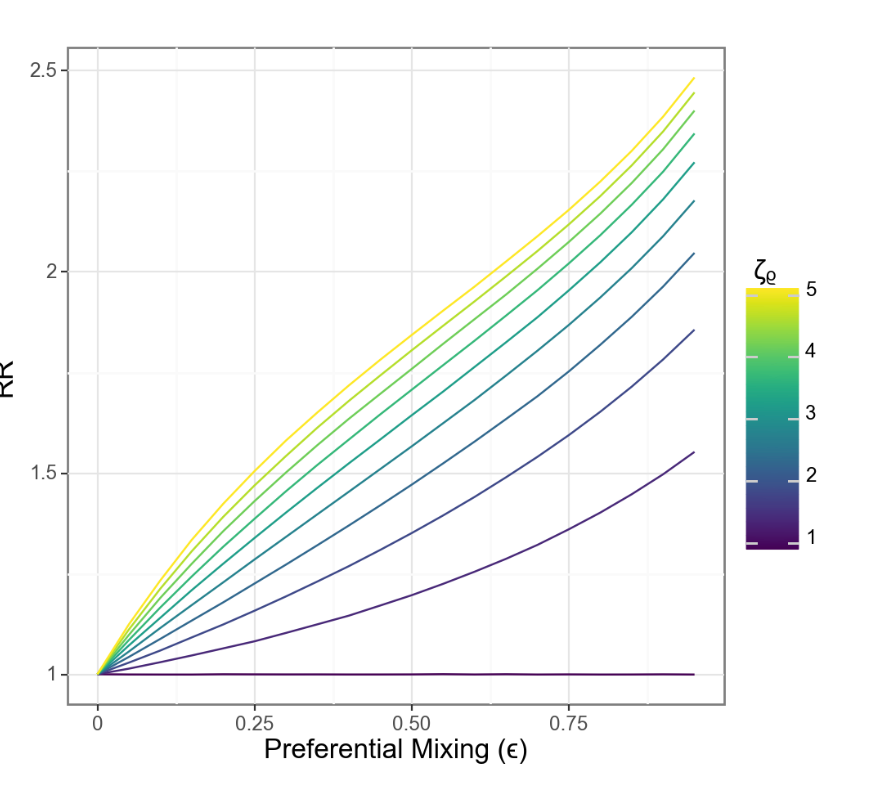
\(\epsilon\) controls spatial dissimilarity, i.e. the degree of within vs. between-group mixing.
Parameter \(\rho \ge 1\) characterizes the change in risk associated with increasing concentration.
Use the spectral approach to estimating \(R_0\) (10) and numerical simulation to understand the implications of these mechanisms.
How does \(R_0\) scale with contact and concentration?
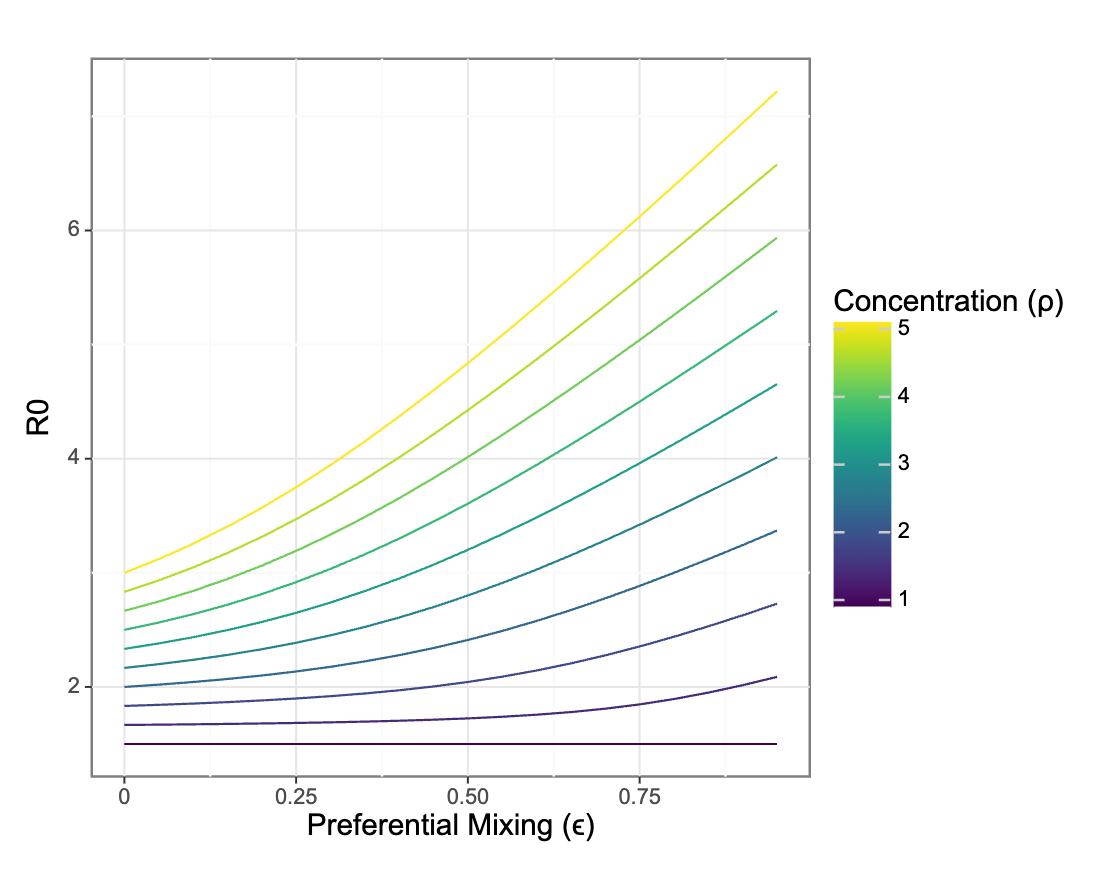
Preferential mixing only impacts R0 in the presence of differential vulnerability to infection between groups
What about relative risks between groups?
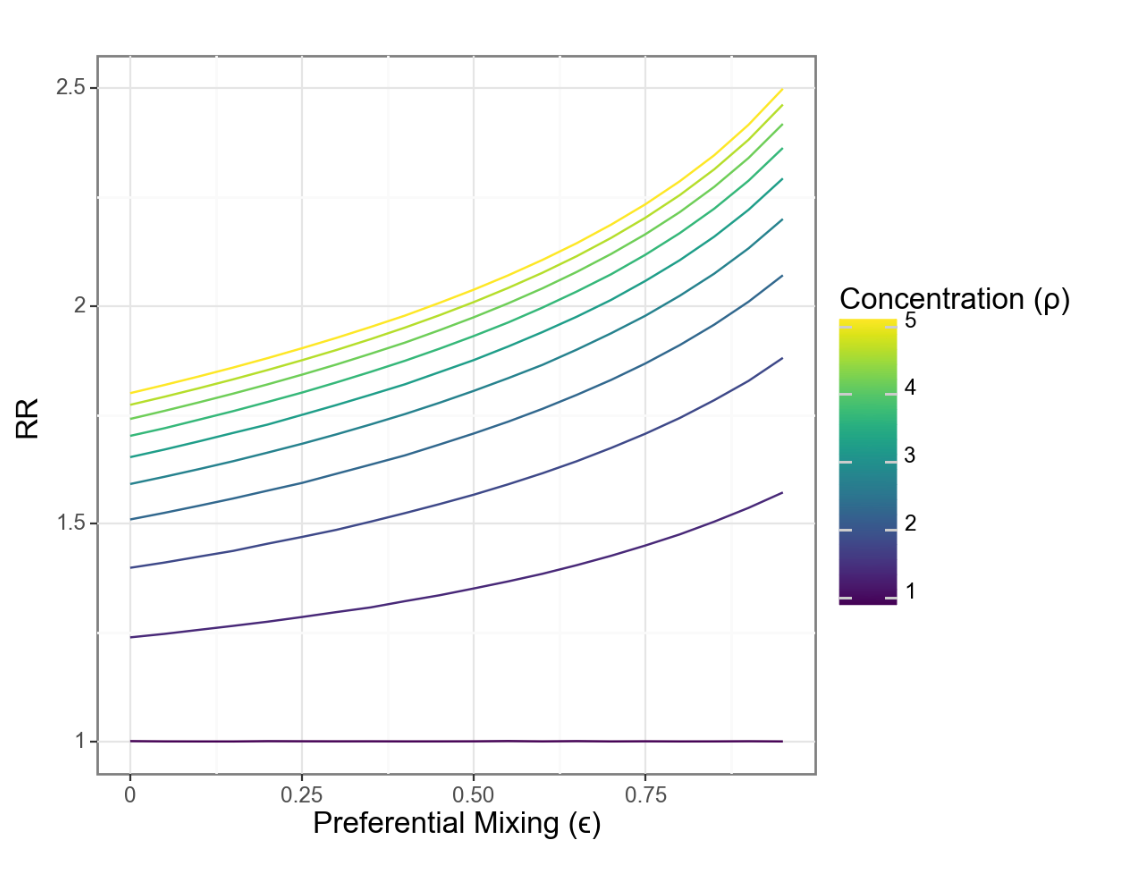
Changes in relative risk are driven by the interaction of concentration and isolation
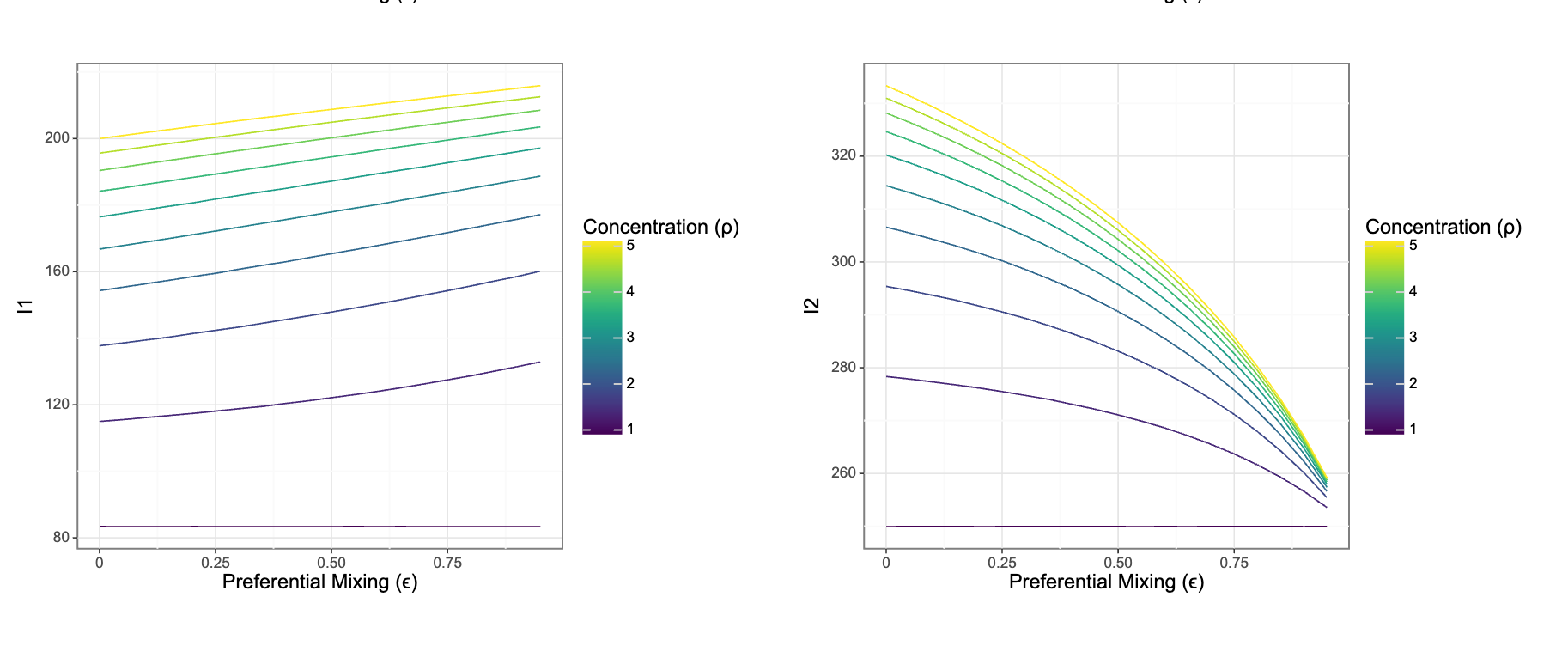
Risks for each group move in different directions even as relative risks grow
A more intuitive relationship?
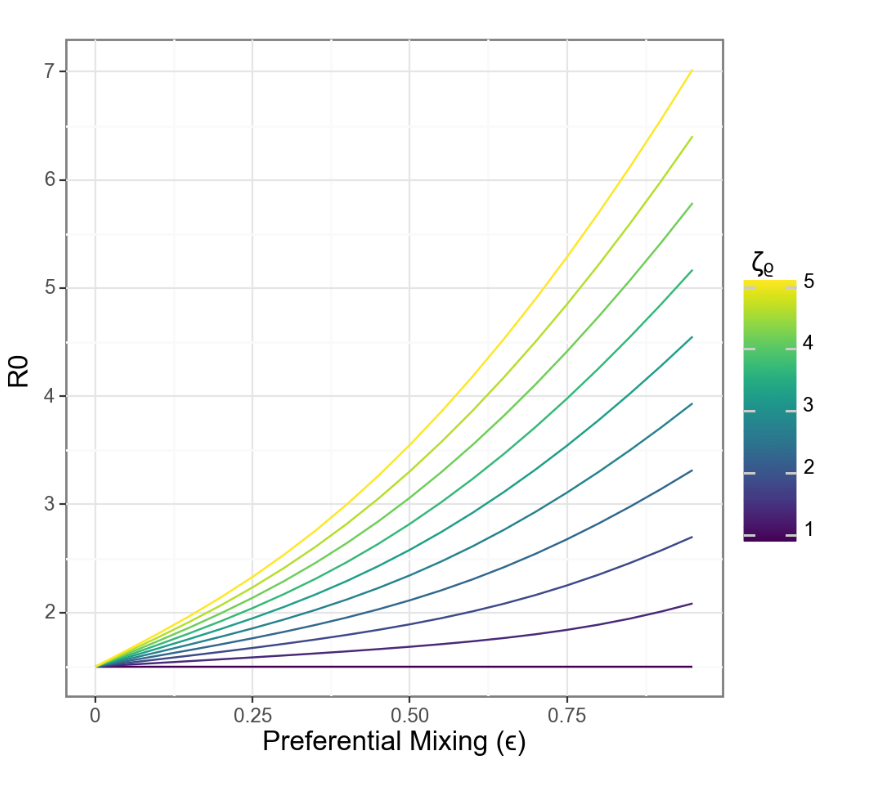
When separation and vulnerability are mechanistically linked, R0 grows linearly with separation
Relative risk also scales more closely with separation
Thanks!
Work supported by NIMHD R01MD017218
For more info abour our research check out epibayes.io
Related tutorials and teaching materials on my blog at zelnotes.io
![]()
Shiny app with an interactive version of this model I have to leave midday tomorrow to hopefully not injure myself at my daughter’s 7th birthday party at a trampoline park.
So: Please send me a note at
jzelner@umich.eduif any of this is of interest and we don’t get to talk!

